

Background: Adolescent/young adult (AYA) Hodgkin lymphoma (HL) is one of the most common cancers in this age group in developed countries. High socioeconomic status, small sibship size and lack of crowding in childhood are risk factors. We also found that among twins, the twin who had more oral exposures in early life was 80% less likely to develop AYA Hodgkin lymphoma. These risk factors are compatible with the hygiene hypothesis. We wanted to further explore additional risk factors consistent with this etiologic model.
Methods: In a case-family control study, we examined past exposure to 12 infections in serum samples from 291 AYA HL cases and 194 of their unaffected family members. Cases were ascertained from the USC International Twin Registry (n=36) and the USC Cancer Surveillance Program (n=255). We measured antibodies to HSV1, HSV2, VZV, EBV, HHV7, HCMV, HHV6, KSHV, T. gondii, H. pylori, Rubella virus and Parvovirus B19 using a multiplex serology bead array (Luminex) (Waterboer Laboratory, German Cancer Research Center). A positive history of exposure to each infection was determined by a titer threshold specific for each infection. We did not examine the association between antibody levels and risk because of the possible impact of AYA HL diagnosis or treatment. We made the assumption that disease or treatment would not affect detection of a low level of antibody indicating previous exposure. A logistic regression model was used to calculate the odds ratio (OR) and 95% Confidence Interval (95% CI) adjusting for age at blood draw, sex and family. The sample was mostly non-Hispanic white, thus we did not adjust for race/ethnicity. We performed stratified analysis for histologic subtype where possible. Linear regression was used to calculate the p-for trend for 0, 1 or 2 fecal-oral or respiratory infections, with 0 infections as the reference.
Results: The mean age at diagnosis in AYA HL cases was 30 years and the mean age at blood draw was 36 years. 57% of the cases were female. Out of the 186 cases with EBV tumor status, 78% were EBV-. Out of the 242 cases with histologic subtype, 72.5% were nodular sclerosis. The mean age of the 194 family controls at blood draw was 53 years and 63.4% were female.
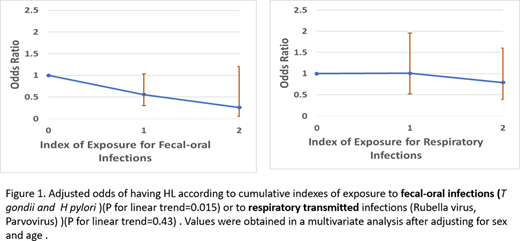
Evidence of past HHV6 infection was associated with an increased risk of AYA HL (OR= 1.80; 95% CI= 1.06-3.07; for nodular sclerosis only: OR= 1.92, 95% CI=1.05-3.42). Having antibodies to H. pylori was associated with a decreased risk (OR= 0.49; 95% CI= 0.25-0.98; for nodular sclerosis only: OR= 0.33, 95% CI= 0.14-0.77). An increasing number of fecal-oral infections (H. pylori, T. gondii) was associated with a decreasing risk of AYA HL (ptrend=0.015), while an increasing number of respiratory transmitted infections (Rubella virus, Parvovirus) was not significantly associated (ptrend=0.43). After adjusting for family, infection with Parvovirus was strongly and significantly associated with AYA HL (OR=3.8,1.06-13.6; for nodular sclerosis only: OR=10.5, 95% CI=1.71-65.25). Past infection with EBV was not associated with risk of overall HL, or with EBV- or EBV+ AYA HL separately, probably because of the high frequency of this infection in the overall population.
Conclusions: We found continuing evidence for an inverse association between fecal-oral transmitted agents and risk of AYA HL, supporting the hypothesis that a deficit of early life fecal-oral transmitted microbes may be associated with susceptibility. HHV6 and Parvovirus were associated with an increased risk, possibly due to a subclinical immune deficiency or another unknown mechanism
No relevant conflicts of interest to declare.

